Medical Health Care Mission In Rojava Planning and Budget For 4-Year Rojava Health Care Mission
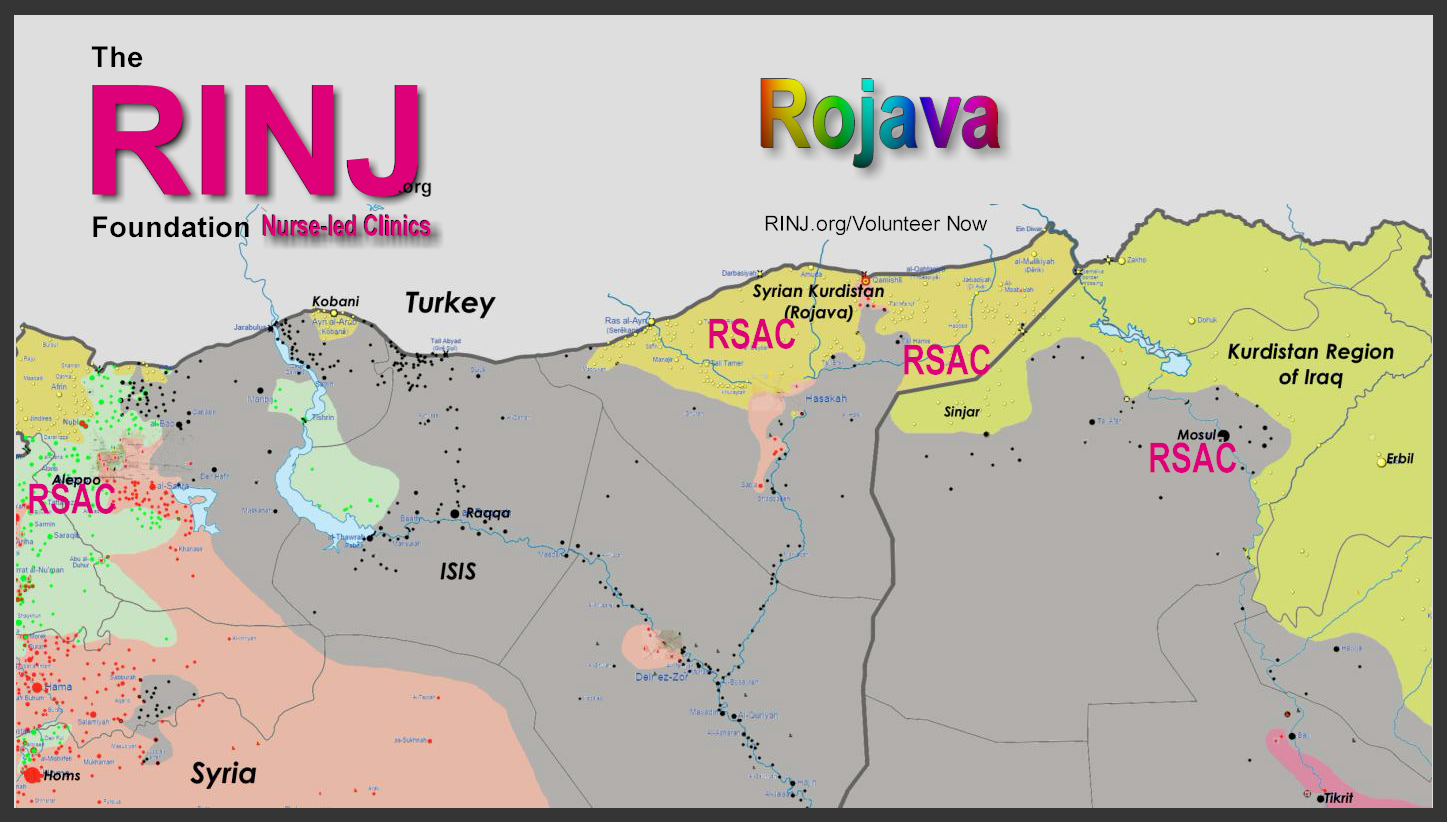
There are roughly ten million displaced persons from and in Syria and 3 million in Iraq. Must they leave their homeland? No. We are kickstarting a program to build 31 clinics across Northern Syria. Please read on.Preamble to the Constitution and Charter of Rojava
We, the people of the Democratic Autonomous Regions of Afrin, Jazira and Kobane, a confederation of Kurds, Arabs, Syrics, Arameans, Turkmen, Armenians and Chechens, freely and solemnly declare and establish this Charter.... this is the region that needs our help.
In pursuit of freedom, justice, dignity and democracy and led by principles of equality and environmental sustainability, the Charter proclaims a new social contract, based upon mutual and peaceful coexistence and understanding between all strands of society. It protects fundamental human rights and liberties and reaffirms the peoples' right to self-determination.
Under the Charter, we, the people of the Autonomous Regions, unite in the spirit of reconciliation, pluralism and democratic participation so that all may express themselves freely in public life. In building a society free from authoritarianism, militarism, centralism and the intervention of religious authority in public affairs, the Charter recognizes Syria's territorial integrity and aspires to maintain domestic and international peace.
In establishing this Charter, we declare a political system and civil administration founded upon a social contract that reconciles the rich mosaic of Syria through a transitional phase from dictatorship, civil war and destruction, to a new democratic society where civic life and social justice are preserved.
What do we do over the next 4 years?
- Initial team of 20 nurses now inbound to brick-and-mortar facility in Kobane.
- Second team of 24 nurses to arrive in later after imaging department tele-health centre built to support regional outposts.
- Nurses will do hospital shifts fit to their RSAC-R1 Facility work schedule
- Delivering Medical services and script fills after 4-days from arrival.
- Hosted by Canton in 1st 4 days while eng. team roughly fixes building and sterilizes nominal facilities in one section of the building while other work continues.
- Two Team Leaders (RN and NP)
- Advance team 20 Nurses
- Edge of city Rojava HQ building, Kobane HQ (Kurdistan)
- The first of thirty regional mobile clinics arrive with varying capabilities - the first units to Sinjar area or the current priority area of thirty villages in Rojava and eastern Kurdistan (KRI - near Dohuk.
- RSAC general health care facilities
will focus on women and children health care including obstetrics, STD's, infectious disease control, pregnancies, general trauma, overall health care. No patient is turned away, some will be escalated to a hospital. - All Patients will Receive Full Care on First Visit
- International research provides clear evidence of the correlation of reliable access to effective practices with better population health outcomes. While it is not always possible for a patient to see her own nurse or her other medical team members, efforts are made to ensure that continuity of care remain central to access planning and quality which is why I favour a small leave-behind presence (Two-Staff, Land Rover and Tent) when the Mobile RSAC moves onward in rotation.
- Establishing wait time targets in basic RSAC care is exceedingly difficult. Therefore, in lieu of setting access targets, we focus on enhancing access, specifically through same-day scheduling for things like pharmacological dispensing, blood tests, inoculations etceteras all done the same day as the face-to-face.
- Demographics of the population such as age, gender, language spoken, culture, socioeconomic status, and medical complexity determine the number of patient visits within a time line. We tend to favour the Murray and Tantau model which leaves 65 per cent of the day's bookings open for walk-ins or deferrals and 35 per cent booked.
- The 35 per cent are for patients who 'couldn't make it in on Friday and chose Saturday instead' or 'patients whom the intake deliberately scheduled today for follow-up'. Direct visits, after-hour appointments, and Smartphone communication or other digital follow up can take up shortfalls. The goal is to see all patients scheduled and unscheduled, avoiding as much as possible, long wait times. That's the basic model.
- We have a performance model for this work and need to see a certain number of patients per month to justify the location. Most return pt visits are weekly. So you see a 20ft Mobile RSAC unit supported by a two-staff, a land-rover and a tent to do follow ups when the Mobile RSAC unit moves to the next camp could well be the precursor to dropping a 40ft RSAC unit if the patient load calls for that. (The 40ft units have triple the staff and can handle four times the number of pts as a 20 ft. RSAC Unit but they can't move and operate 24/7)
- Until we have enough units in the field
every five days we make a move - the 20 ft. Units are good for this. The follow ups are pt progress and treatment monitoring. Procedures are only done in the Mobile Units. We really do want to stick to our mission and don't want to get into a bog where we are locked down doing general practice work only. We in this manner focus on finding and regularly seeing as many sexual violence pts as we can. We prevent suicides, quash the spread of dangerous STDs, and collect sexual-violence testimonial and forensic evidence related to law enforcement; and everyone is better served by that focus. - The 20 foot units have a 55 gallon water tank and pump system. This allows for one week of water supply at normal usage. Water must be obtained and purified once a week and this is the job of the administrative person.
- The split a/c is D/C inverted and very efficient. All equipment and lighting is universal power with universal outlets. Solar equipment/system can be programmed for 110 volt - 220 volt 50/60 hz. There are six solar panels that can be permanently mounted on the roof which can produce 1500 watts of electricity. There are eight sealed lead-acid solar batteries which is the primary source of stored power. The whole clinic's average power consumption with all equipment on (including a/c unit) is 500 watts. Even on a rainy/cloudy day our supply verses demand of power is usually 4:1 ratio.
- Every surface can be disinfected. We use Parkland Plastic Non-frp on the ceilings and the walls. The flooring is Armstrong seamless vinyl and is coved up the walls 3 inches. There is four inches of 1/2 lb icynene expandable foam insulation in the walls and ceilings which in effect gives you a R16 value. Electrical is to international code. Walls are steel studded and Everything is level 1 commercial product. Meaning we have designed our units to be very durable to withstand the most austere environments.
- More information:
https://therinjfoundationfreeposters.wordpress.com/rinj-rsac- mobile-clinics-for-kurdistan- iraq-and-various-african- nations/
{kind=link}
{kind=link}
{kind=link}
Budgets and Costs
(Money is in $USD and Year-Dollars are 2016)- Each clinic has a total need of:
- $52k x 5 (3 Nurses, 2 security/assistants)
- $35k x 1 Health Care Administrator (Certificate)
- $3500 x 3 Regional volunteers who speak the language of the locals.
- $52K Meds we must buy
- $20K Equipment maint., spares, O2, disposables.
- 377,500 Per year Per Unit
- 30 Mobile Clinics for Delivery of Medical Services, Including Treatment of Rape Survivors, in The Rojava Districts of Syria Incl. Initial cost per 20ft. clinic is about $70k and shipping is $5k. This concept is designed to use thirty 20-ft containers, converted into mobile self-contained one room medical clinics, as a means of providing medical services including treatment of rape survivors to the autonomous region of northern Syria known as Rojava. These mobile clinics are desperately needed by the people of Rojava since much of the area's medical infrastructure has been devastated by three years of the Syrian Civil War and two years of fighting the Islamic State terrorist group. * Total Project Amount: $47,550,000. * Total Project Duration: 48 months
{kind=link}
We are The RINJ Foundation an international NGO Providing Nurse-Led Medical Services For Women and Children. (RSAC) The RSACs offer free medical care and community related services such as general medicine, general health care, survivor advocacy, crisis and mass trauma surge capacity, community outreach, & education programs are provided based on each RSAC's resources at the discretion of the local RSAC nurse-led team.
We are in Kurdistan and are undertaking an ambitious program to provide health care to thousands of refugees and returning displaced persons. We are looking for serious funding assistance for an aggressive program to provide health care in Northern Syria to Kurdish and Yazidi peoples.
- Each clinic has a total need of:
- $52k x 5 (3 Nurses, 2 security/assistants cost-to-support-plus monthly stypen)
- $35k x 1 Health Care Administrator (Certificate / cost-to-support-plus monthly stypen)
- $3500 x 3 Regional volunteers who speak the language of the locals (cost-to-support).
- $52K Meds we must buy
- $20K Equipment maint., spares, O2, disposables.
- 377,500 Per year Per Unit (Would you sponsor a unit?)
- 30 Mobile Clinics for Delivery of Medical Services in The Rojava Districts of Syria Incl. Initial cost per 20ft. clinic is about $70k and shipping is $5k. This concept is designed to use thirty 20-ft containers, converted into mobile self-contained one room medical clinics, as a means of providing medical services including treatment of rape survivors to the autonomous region of northern Syria known as Rojava. These mobile clinics are desperately needed by the people of Rojava since much of the area's medical infrastructure has been devastated by three years of the Syrian Civil War and two years of fighting the Islamic State terrorist group. * Total Project Amount: $47,550,000. * Total Project Duration: 48 months
The RINJ Foundation's women's health care nurses at RSAC facilities provide a full range of outpatient & walk-in health care services to patients and provide special care to GBV survivors, infectious disease control cases, pregnancies, small children etc..
- Trauma care;
- Physical injuries treatment and minor surgery;
- Sexually transmitted disease detection treatment and prevention;
- Sexual assault forensic testing;
- Pregnancy issues, from abortion to delivering your baby;
- Legal course of action counselling;
- Criminal prosecution assistance;
- Mental health care; and
- all needed follow-up care.
Nurses And Other Medical Staff - Volunteers
Human Resources and Volunteer FormMedical Standards Documents