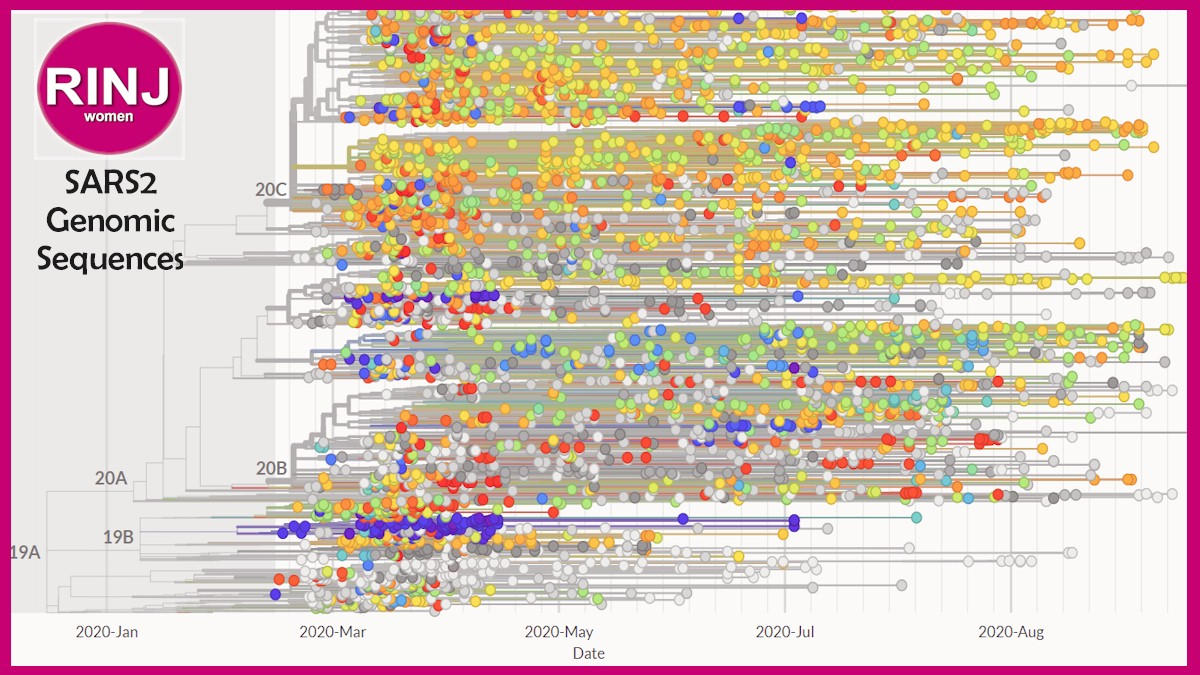
North America SARS2 Genomic Sequences
source: Nextstrain
Anecdotally on medical networks, practitioners are talking about hundreds of COVID-19 reinfection cases, and they are bad.
The CEO of The RINJ Foundation has issued a warning memo to all practitioners, interns and administrators about the perils of patients/clients ignoring indications of chronic illness.
Because lack of CoV reinfection indication of former mild cases may lead to serious consequences in that millions of unknown mild cases reinfected with COVID-19 may have higher IFR.
The warning suggests that early indications of incipient chronic illness must be treated or the disease could become a comorbid factor to a low-viral load or mild-response SARS-CoV-2 infection, all later (4-9 months) becoming an underlying set of vulnerabilities to a COVID-19 reinfection with a fatal outcome.
RINJ.org is a member of the Civil Society Partners for SARS-CoV-2 Pandemic Solidarity
“Alcoholism, drug addiction, obesity, asthma and chronic lung disease, hypertensive and other heart diseases, diabetics and pre-diabetes, must be treated and brought under control,” says Micheal O’Brien, the CEO of the global civil society NGO.
“Patients must be discouraged from a laissez faire attitude toward treatment of chronic illness,” he told Michele Francis and her cohorts in Venezuela.
“We lost a patient in June,” reported the CEO, “a gentleman who refused to take his antihypertensive medications. Following case reviews a general suspicion about the case that patient attitude was an indicator for an additional specialized medical response—a stricter adherence to mental health indications from health workers. Hence the suggestion has been made that counseling for patients who demonstrate lax attitudes toward chronic noncommunicable disease is now indicated during the COVID-19 pandemic.”
Dr. Anna Wachtel, a New York City MD specialized in psychiatry noted in a ‘doctors-medical-network (Doximity)’ discussion of SARS-CoV2 reinfections that, “We often forget those other illnesses that weaken immune systems and make the body more prone for infection or RE-infection. Alcohol use disorder, that is so common in US and other countries among young adults and adults, offer a free entry to virus or bacterial respiratory infections that as well might have a multi organ presentation as it’s developing. … Untreated depression , anxiety, bipolar disorder …. [they] lower your immune system by scientifically proven ways…Personality disorders that are often undiagnosed or misdiagnosed or not treated properly can contribute to above mentioned disorders and viral infection that can have a severe presentation.” (Citing Dr. Anna Wachtel NYC/NY/USA)
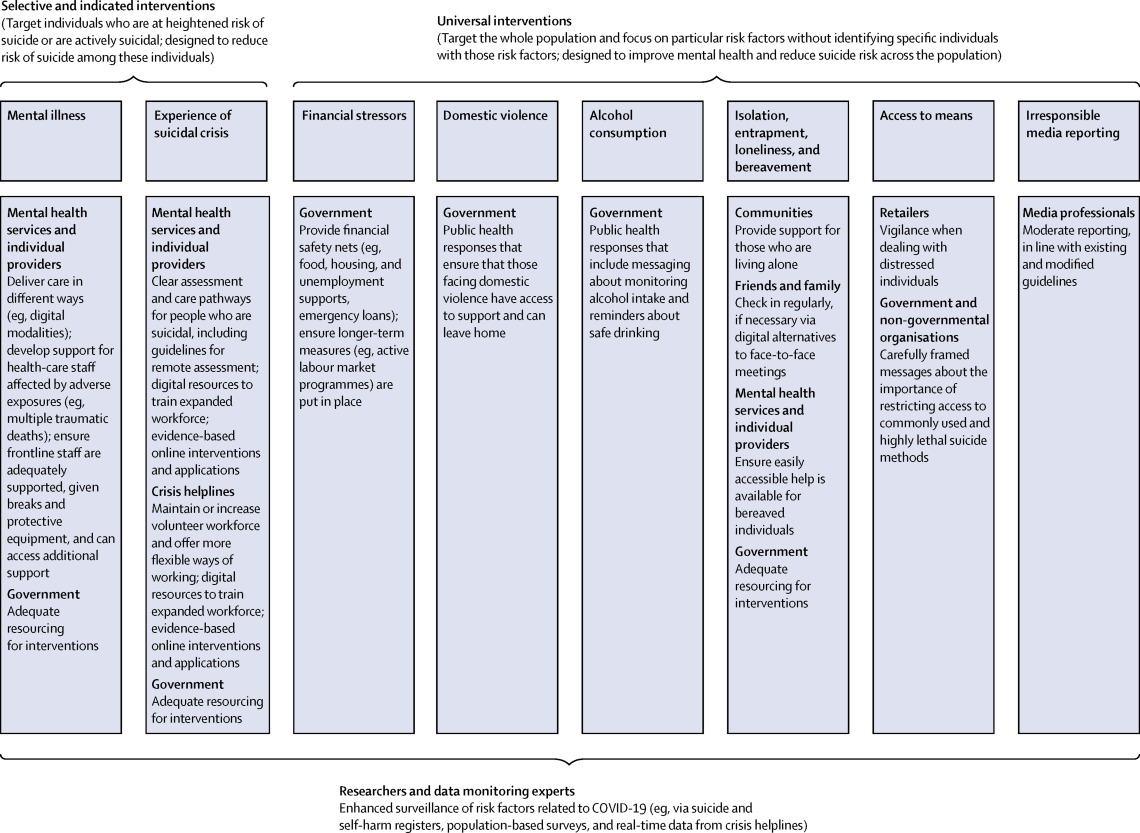
Click to enlarge. From The Lancet Coronavirus Resource Center for Practitioners
SARS2 Reinfection is a complicated issue because for longtimers, COVID-19 becomes a comorbid illness unto itself.
“Examining the range of slightly varying reported genome sequences of the SARS2 virus,” noted both authors, O’Brien and Harris (Harris leads the Civil Society Partners for COVID-19 Pandemic Solidarity pandemic tracking team), “the significance of reinfection is less about antibodies and more about cell damage creating new comorbid illness.”
“It is a paradox: a very old, stable virus yet to humans a ‘novel’ coronavirus,” noted the two directors in a joint memo circulated globally.
As antibodies vanish, reinfection with SARS-CoV-2 creates a new comorbid underlying illness in addition to those that exist—COVID-19 itself—because of the cell damage each infection causes.
This could raise the IFR and create an endless recycling pandemic until there are no more vulnerable humans that SARS2 is able to infect.
(Join the latter group by treating chronic illness and having pts wear a fit tested N95 mask instead of a flimsy piece of cloth draped across the mouth under the nose as is seen in the small USA mask wearing population.)
The importance of some recent known SARS2 reinfection discoveries indicate an ominous potential danger.
“The virus is in the incipient stages of cycling through previously infected population. As it does so it will be worse because any person who has been infected previously may have hidden or even symptomatic chronic illness caused by cells damaged by SARS2,” explains Fred Harris, the bio-statistician team lead of the Civil Society Partners for COVID-19 Solidarity in Singapore.
Scientists evaluating the first known reinfection in the United States explain, “What is worrisome is that SARS-CoV-2 reinfection resulted in worse disease than did the first infection, requiring oxygen support and hospitalization. The patient had positive antibodies after the reinfection, but whether he had pre-existing antibody after the first infection is unknown.”
The other worrisome factor is the enormous number of patients (maybe 20% of USA population) whose first infection produced none or only mild symptoms.
Cell damage exists; antibodies dissipate fast; and T-cells are no more robust for the minor course of infection.
Problem: these patients maybe the younger ones now presenting with serious symptoms, comprising the new, higher CFR among the young demographic.
Question: how many reinfection kill a healthy young patient? We may not know until around 2024 if 8 months is a realistic expectation of post-infection antibodies and 2 years is an accurate estimate for long-timers’ cell-damage and even incipient thrombosis intervention or recovery.
If SARS-CoV-2 recycles through large populations every 9-12 months, USA had the worst possible Phase 1. Doctors Birx and Fauci are then correct, this is the poorest possible situation.
Known Reinfections present Worrisome Outcomes
“Richard L Tillett and colleagues describe the first confirmed case of SARS-CoV-2 reinfection in the USA.2 A 25-year-old man from the US state of Nevada, who had no known immune disorders, had PCR-confirmed SARS-CoV-2 infection in April, 2020 (cycle threshold [Ct] value 35·24; specimen A). He recovered in quarantine, testing negative by RT-PCR at two consecutive time points thereafter. However, 48 days after the initial test, the patient tested positive again by RT-PCR (Ct value 35·31; specimen B). Viral genome sequencing showed that both specimens A and B belonged to clade 20C, a predominant clade seen in northern Nevada. However, the genome sequences of isolates from the first infection (specimen A) and reinfection (specimen B) differed significantly, making the chance of the virus being from the same infection small. What is worrisome is that SARS-CoV-2 reinfection resulted in worse disease than did the first infection, requiring oxygen support and hospitalisation. The patient had positive antibodies after the reinfection, but whether he had pre-existing antibody after the first infection is unknown.”
Characteristics associated with reinfection with SARS-CoV-2
| Location | Gender | Age | 1st infected (ct) | 2nd (ct) | Days Between | Antibody after 2nd |
| Hong Kong | Male | 33 | Mild (N/A) | Asymptomatic (27) | 142 | IgG+ |
| Nevada, USA | Male | 25 | Mild (35) | Hospitalised (35) | 48 | IgM+ and IgG+ |
| Belgium | Female | 51 | Mild (26–27) | Milder (33) | 93 | IgG+ |
| Ecuador | Male | 46 | Mild (37) | Worse (N/A) | 63 | IgM+ and IgG+ |
viral genome sequences. Ct=cycle threshold. N/A=not available.
SARS-CoV-2=severe acute respiratory syndrome coronavirus 2.
Reinfections of COVID-19 are now being tracked around the world. This indicates a cyclical community spread of COVID-19 as warned of in previous articles by the biostatisticians on the Civil Society COVID-19 Solidarity Team.
Take a self-training video course on wearing a mask.
Wear a Mask Every time you go out.
 Photo credit: Micheal John/FPMag One of many types of medical masks.
Photo credit: Micheal John/FPMag One of many types of medical masks.
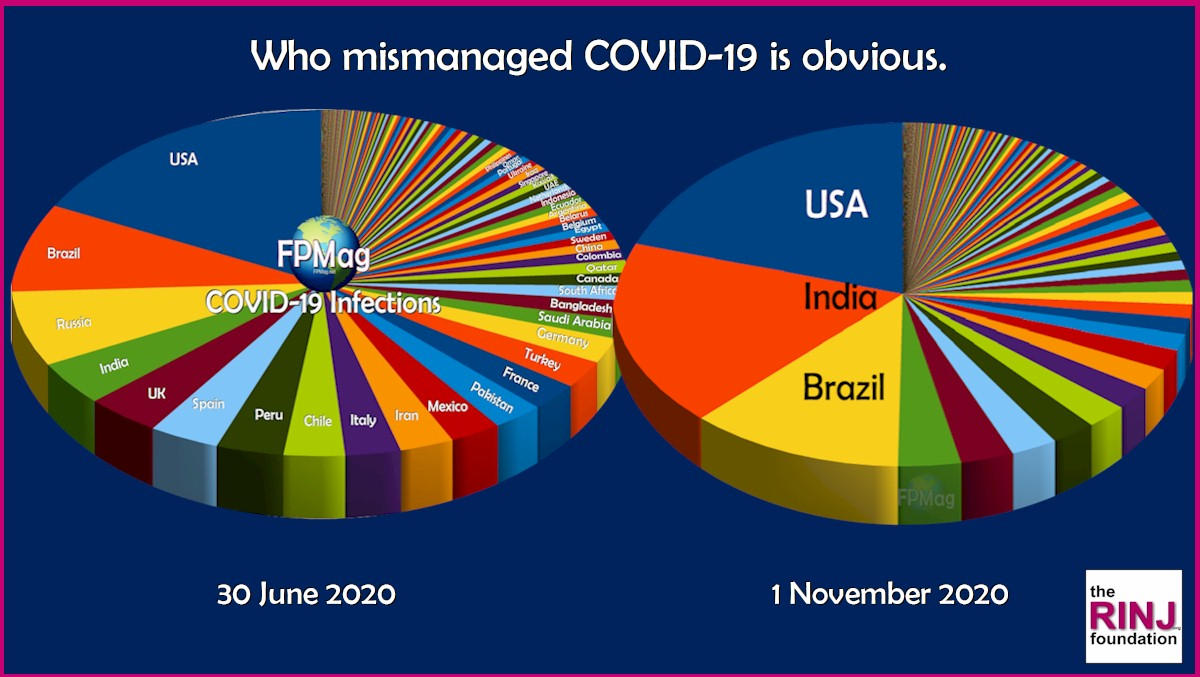
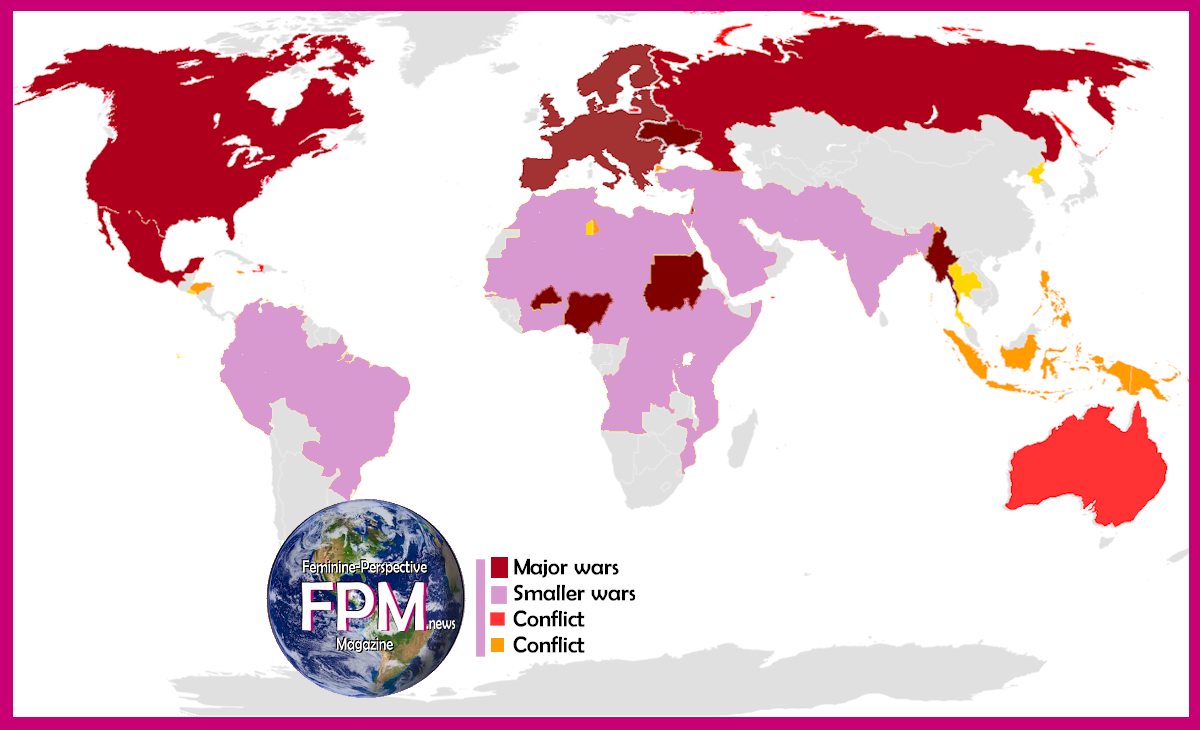
Distribution of disease (COVID-19) infections from June 30 to 1 November 2020.









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}