By Michael Head, University of Southampton
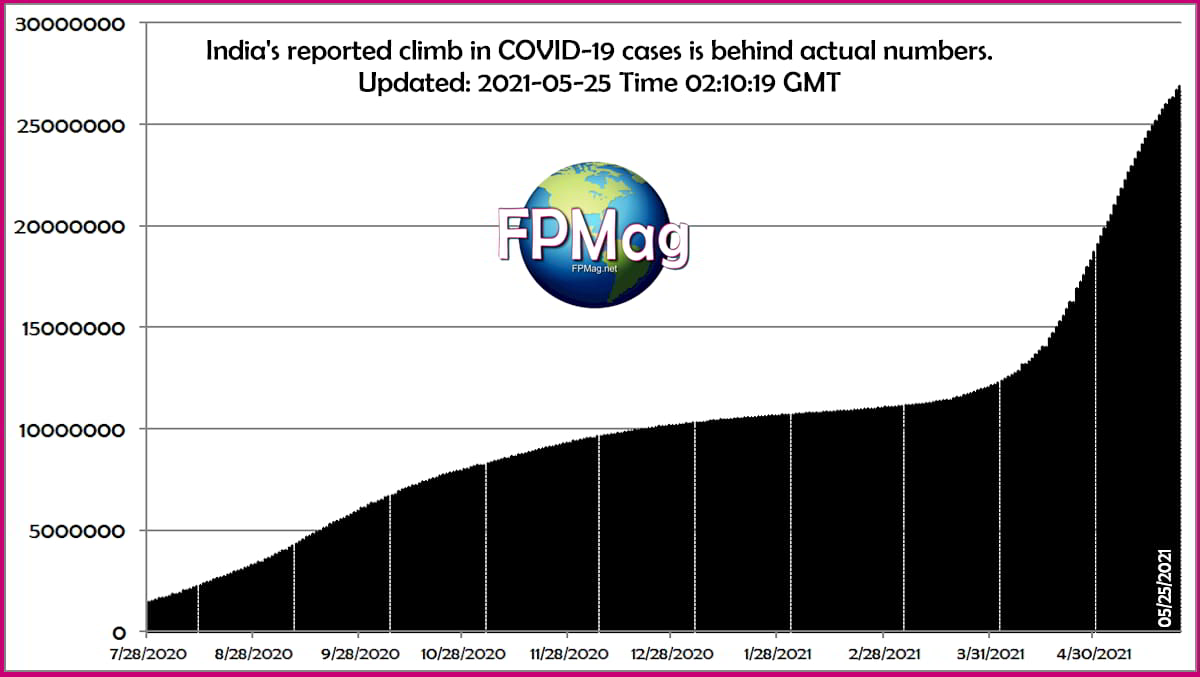
India’s steady climb in cases. Source: CSPaC
Beneath the many complexities of the marathon that is the COVID-19 pandemic, there is a simple hypothesis: if the coronavirus is introduced into a susceptible population, and those people are able to mix, then there will be significant community transmission. Across 2020 and 2021, we have seen this happen around the world, including, recently, in India.
Could we see further situations like those in India, with cases rapidly spiking and health systems being overwhelmed? The short answer, sadly, is yes.
Globally, there’s been an encouraging downturn in daily new cases in May 2021, but despite this, cases are still at a very high level overall, with worldwide statistics masking huge differences across countries and areas. The global vaccine rollout is also progressing slowly, with most of the world still susceptible to COVID-19. These factors mean there’s potential for further spikes like those seen in India.
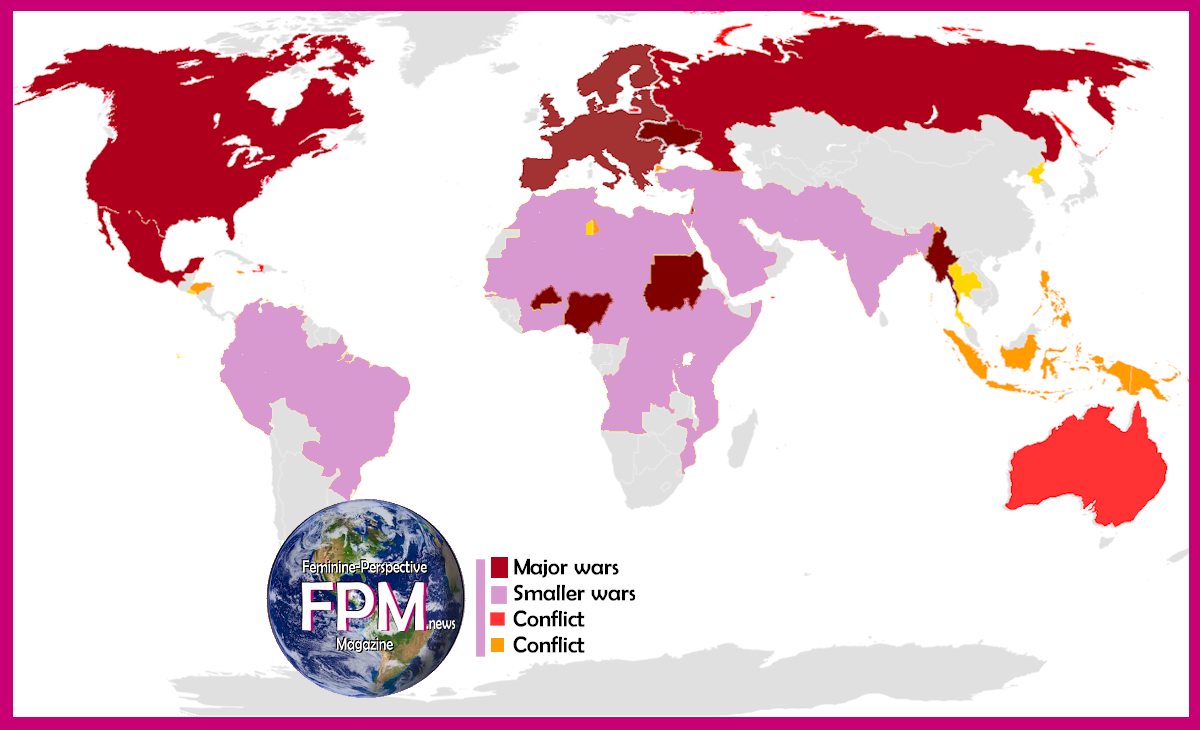
We only need look to Nepal to see a similar situation unfolding. Other countries have rising caseloads too, with many eyes looking nervously at Latin America, south-east Asia and some of the smaller island nations.
Who else is at risk?
In terms of where cases are increasing most quickly (at time of publication), the website Our World in Data highlights Laos, Timor, Thailand, Cambodia, Fiji and Mongolia as the countries where numbers have recently doubled in the shortest period of time (ranging from 16 to 23 days for these countries; for comparison, the doubling rate for India ahead of its second wave was 43 days). When looking at the countries whose reported deaths are currently doubling most quickly, it’s Timor, Thailand, Mongolia, Cambodia and Uruguay (range: four to 31 days).
For countries such as Laos, Thailand, Cambodia and also Vietnam (highly praised so far), it’s high susceptibility to COVID-19 that’s the problem. They’ve had few cases in the past, so there’s little natural immunity, and they’re now experiencing outbreaks amid an inability to procure a large vaccine supply. Vaccine coverage therefore is low. Thailand and Vietnam have given a first dose to just 2% and 1% of their populations respectively.
Elsewhere, it’s the mixing part of the equation that’s more of a concern. Japan, for example, is soon to host the Olympics, attracting athletes, dignitaries, coaches and media from every corner of the globe. Despite a ramping up of vaccine distribution over the past month, the programme has been sluggish, with less than 4% of the population having received a first dose. In this author’s view, the Olympics should not go ahead this year.
Latin America continues to experience a huge burden of COVID-19 disease and so is also at risk. Argentina, Uruguay, Costa Rica and Colombia are all still in the top ten countries in terms of daily new confirmed cases per million people. On the other hand, sub-Saharan Africa has on the face of it – with some exceptions – handled the pandemic relatively well, with countries praised for an early and decisive response, having learned lessons from the west African Ebola outbreak of 2013-16.
Working with uncertain data
Of course, our conclusions must be cautious. Creating high-quality real-time data during a public health emergency is complicated, and data is patchy and slow in most parts of the world. The extent of transmission within refugee camps and in conflict settings, for instance, is very much unknown. Some vulnerable areas may slip under the radar.
The reporting of data may also be influenced by local politics. Some countries, such as Tanzania, have chosen to downplay the severity of COVID-19. The former Tanzanian president, John Magufuli, died in March 2021 – and news coverage suggested he may have died of COVID-19 amid reports of uncontrolled outbreaks around the country and sharp increases in deaths. However, officially the impact of COVID-19 in Tanzania has been low.
Similarly, Belarus is reporting low death rates (27.8 per 100,000), having refused to consider COVID-19 a serious threat. But the Institute for Health Metrics and Evaluation (IMHE) has modelled the country’s actual death rate to be one of the highest in the world, at 472.2 per 100,000 people. IHME modelling puts Azerbaijan at the top of that list, with a death rate of 672.7 compared with official numbers of 46.3 per 100,000.
Politics and mixing
The timing of elections and volatility of political governance may be interesting factors to observe when trying to predict future spikes in cases. Political mass gatherings in India are likely to have contributed to the extensive recent transmission. The prime minister and health minister encouraged people to attend, wrongly believing earlier in the spring that India had reached the end stages of the pandemic.
Elsewhere, Donald Trump’s campaigning events caused numerous super-spreading events in the US, while in Myanmar there were reported breaches of COVID-19 protocols due to electioneering and mass gatherings. Myanmar’s elections in October 2020 were preceded by the highest spike in cases the country had experienced. Soon after the election, stricter policies were put in place and case rates lowered. Countries that engage in similar behaviour – or, like India, declare success too early – could well be the next hotspots.
Of course, the next outbreak may prove difficult to spot. Few of us could easily point to Timor on a map. This lack of knowledge influences our perception over local situations and also the news coverage that countries get. Compare Nepal and Timor to Brazil and India, on which public reporting has been extensive. Plus, some countries might not be reporting good-quality data – Belarus, Azerbaijan or indeed Russia may have much bigger burdens of COVID-19 than appears to be the case.
The “next big outbreak” will be reliant on a perfect storm of a few variables coming together. At the core of this storm will be a slow vaccine rollout and susceptible populations mixing freely. Political rallies, large-scale festivals and protests are examples of mass gatherings that can seed new outbreaks and facilitate sufficient spread to rapidly overwhelm a health system. But depending on where this happens, we may not even notice.![]()
Michael Head, Senior Research Fellow in Global Health, University of Southampton
This article is republished from The Conversation under a Creative Commons license. Read the original article.
04/20/2024
Below: CSPAD estimated 2024-04-19 22:12 GMT COVID-19 data for India.
EPICENTER-2: India (45,035,393)
| Reported | *Cases | *Deaths | *CFR | *Recovered |
| India | 45,035,393 | 533,570 | 1.2% | 0 |
Note: India's reported death sum and cured data are widely seen among epidemiologists and biostatisticians as unreliable. For example, 3,094,653 is CSPAD estimated sum of deaths while India reports 533,570, creating the largest discepency in the world. India might only report hospital tested cases. Sources among hundreds of nurses and other medical practitioners provide a picture that in summary concludes most cases never present in a hospital especially in northern provinces where health care is less available and utilization is low anyway because of poverty, hence most people die at home in India. This theory could explain discrepancies between reported data and algorithmic estimates.
| Locale | Cases | Deaths | Active |
| India reported: | 45,035,393 | 533,570 | 44,501,823 |
| India estimates: | 249,045,723 | 3,094,653 | 245,951,070 |
Data collected and reported by: Civil Society Solidarity Partners against Disease









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}